Imagine yourself seated in a chair breathing comfortably in and out. The amount of air you are moving is called the "tidal volume" and for an adult it is give or take 500 ml. How does your body know what is a "comfortable" amount of air... how does it decide how big your tidal volume should be? The answer is your tidal volume is going to be the amount of air that is most efficient for you to move.
The lungs sit in your chest and stay in place because they're stuck to structures in the hilum. But apart from that they float in pleural fluid that (by means of capillarity) stick the outer covering of the lung to the inner layer of the chest. At the end of a breath, during that moment when no energy is being exerted and nothing is moving, all pressures in the lung are at zero. In order to draw the next breath, the diaphragm drops increasing the volume of the thorax. In so doing, negative alveolar pressure develops that "sucks" air into the lungs. During expiration the reverse happens. The diaphragm relaxes and rises, decreasing the size of the thorax, increasing pressure exerted against the alveoli, pushing air out of the lung and chest. So what factors determine how much air goes in and comes out of the lung with each breath? There are basically two. One is how stiff the chest wall or lung tissue is (this is called "compliance") and how much airway pressure there is. If airways are narrow, it will take more pressure to get air to move through them.
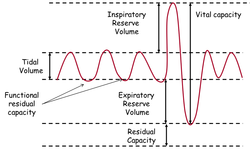
That brings us back to you sitting in a chair breathing quietly in and out. Look at the diagram above. Find the squiggly line labeled "tidal volume". That's the volume/amount of air that goes in and out during a quiet respiration. Now look at the bottom of the squiggly line where the lungs pause before the next breath. The volume at the end of the cycle represents the balance point of all the elasticity in the lung tissue and chest wall. This balance point is also determined by how open and accommodating the airways are. We call this point in cycle the "functional residual capacity"... a very important little number when it comes to the work of breathing!
The lungs sit in your chest and stay in place because they're stuck to structures in the hilum. But apart from that they float in pleural fluid that (by means of capillarity) stick the outer covering of the lung to the inner layer of the chest. At the end of a breath, during that moment when no energy is being exerted and nothing is moving, all pressures in the lung are at zero. In order to draw the next breath, the diaphragm drops increasing the volume of the thorax. In so doing, negative alveolar pressure develops that "sucks" air into the lungs. During expiration the reverse happens. The diaphragm relaxes and rises, decreasing the size of the thorax, increasing pressure exerted against the alveoli, pushing air out of the lung and chest. So what factors determine how much air goes in and comes out of the lung with each breath? There are basically two. One is how stiff the chest wall or lung tissue is (this is called "compliance") and how much airway pressure there is. If airways are narrow, it will take more pressure to get air to move through them.
That brings us back to you sitting in a chair breathing quietly in and out. Look at the diagram above. Find the squiggly line labeled "tidal volume". That's the volume/amount of air that goes in and out during a quiet respiration. Now look at the bottom of the squiggly line where the lungs pause before the next breath. The volume at the end of the cycle represents the balance point of all the elasticity in the lung tissue and chest wall. This balance point is also determined by how open and accommodating the airways are. We call this point in cycle the "functional residual capacity"... a very important little number when it comes to the work of breathing!
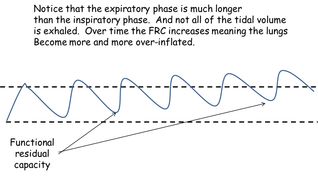
We know that in COPD, patients have clogged, damaged, inflamed airways. Meaning of course that there is increased resistance to airflow. This is mostly a problem during exhalation, however, not inhalation. It's a problem that keeps the the lung from fully emptying out during each respiratory cycle. In the diagram to the left you'll notice two things. First the expiratory phase is very much prolonged compared to inspiration. Second, you'll notice that, over time, air is trapped in the lung and the FRC gradually increases. This is very bad for ventilatory mechanics. To appreciate this fact, take a breath and only let half of it out. Now try to resume "normal" respirations. You'll immediately notice how fatiguing this is. When the COPD patient's lungs are over-inflated, the diaphragms are flattened and don't contribute much to ventilatory effort. The chest becomes barrel shaped. The only way the patient can move air in is to use the muscles that lift the chest out and up. These are the "accessory muscles" of respiration (trapezius and sternoclaidomastoids). This is why COPD patients seem to have big thick layers of muscle extending from their shoulders to their head on either side. In addition, the patient has to struggle to get as much air out as possible before he takes his next breath. In order to do this, the patient has to use his abdominal muscles to push air out... again causing a huge increase in the amount of energy required to breathe.
The patient is not moving much air in the alveoli. This means that there is not much new oxygen available to the RBC's. Not only that, this air-trapping causes alveolar hypoventilation. Now pay attention!!! Whenever there is alveolar hypoventilation, there is hypercapnea (build up of CO2.) And whenever there is a build up of CO2, the reason is always alveolar hypoventilation!!! Yes it's true that CO2 diffuses 20 times more readily than does oxygen. But not when air is not moving into and out of the alveoli. Remember, CO2 from the body is always being delivered to the alveoli via the pulmonary artery and the capillary beds that supply alveoli. If it isn't blown out with each respiratory cycle, it accumulates. What is the result? Increased PaCO2 in the blood gas. Chronic respiratory acidosis, and over time, bicarbonate retention by the kidney. This is an attempt by the body to adjust to the chronic build up of carbonic acid in the blood.
The patient is not moving much air in the alveoli. This means that there is not much new oxygen available to the RBC's. Not only that, this air-trapping causes alveolar hypoventilation. Now pay attention!!! Whenever there is alveolar hypoventilation, there is hypercapnea (build up of CO2.) And whenever there is a build up of CO2, the reason is always alveolar hypoventilation!!! Yes it's true that CO2 diffuses 20 times more readily than does oxygen. But not when air is not moving into and out of the alveoli. Remember, CO2 from the body is always being delivered to the alveoli via the pulmonary artery and the capillary beds that supply alveoli. If it isn't blown out with each respiratory cycle, it accumulates. What is the result? Increased PaCO2 in the blood gas. Chronic respiratory acidosis, and over time, bicarbonate retention by the kidney. This is an attempt by the body to adjust to the chronic build up of carbonic acid in the blood.
