Defining "Pneumonia":
We should probably begin by defining what pneumonia is. The simplest definition of pneumonia an infection with inflammation of lung parenchyma. Time out: What is parenchyma: It's the functional unit of an organ system. A tissue is made up of stroma (the supporting structures of an organ) and parenchyma. The kidney for example is made up of millions of nephrons that are arranged and organized by kidney stroma. The interesting thing about the lung is that it is almost all parenchyma. Cut a lung open and look at it under a microscope and you see alveoli and capillaries. The stretchiness of the alveolar tissues pretty much hold the lung together rather than a basement membrane or organized stroma. Great. So we can just as accurately define pneumonia as an infection of an area of alveoli which fill with inflammatory "juices" (dead micro-organisms, white blood cells, plasma proteins and other inflammatory products) filling the air spaces causing them to collapse and become airless. This solid, airless, inflammed area of lung is said to be "consolidated".
How is Pneumonia Classified?
The classification of pneumonia is a mess.
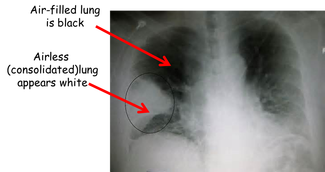
Sometimes pneumonia is referred to by it's location within the lungs. Since the pneumonia in the picture to the left involves an entire lobe of the lung, it might be called "lobar pneumonia". Sometimes it's described by the causative organism. (This x-ray could be showing a "streptococcal pneumonia" for example.) Other times pneumonia is categorized by the event that brought it on. (For example, the patient in the scenario has "aspiration pneumonia")
But, the most important way in which pneumonia is classified is by where the pneumonia was acquired. For example, community acqured pneumonia (CAP) is presumed to be caused by organisms distinct from those that cause hospital acquired pneumonia (HAP). HAP is usually the result of infection with resistant organisms that are beginning plague acute care facilities. These include methicillin resistant staphylococcal aureus (MRSA) or the gram negative bacteria pseudomonas aeruginosa. Another type of pneumonia, one considered as a quality indicator for health care facilities, is ventilator acquired pneumonia (VAP). Since the advent of powerful oral antibiotics, progressively earlier discharge from hospitals, and the use of infusion centers for antibiotic therapy more drug resistant organisms are occurring in the community. These are referred to as health-care associated pneumonia (HCAP).
Sometimes pneumonia is referred to by it's location within the lungs. Since the pneumonia in the picture to the left involves an entire lobe of the lung, it might be called "lobar pneumonia". Sometimes it's described by the causative organism. (This x-ray could be showing a "streptococcal pneumonia" for example.) Other times pneumonia is categorized by the event that brought it on. (For example, the patient in the scenario has "aspiration pneumonia")
But, the most important way in which pneumonia is classified is by where the pneumonia was acquired. For example, community acqured pneumonia (CAP) is presumed to be caused by organisms distinct from those that cause hospital acquired pneumonia (HAP). HAP is usually the result of infection with resistant organisms that are beginning plague acute care facilities. These include methicillin resistant staphylococcal aureus (MRSA) or the gram negative bacteria pseudomonas aeruginosa. Another type of pneumonia, one considered as a quality indicator for health care facilities, is ventilator acquired pneumonia (VAP). Since the advent of powerful oral antibiotics, progressively earlier discharge from hospitals, and the use of infusion centers for antibiotic therapy more drug resistant organisms are occurring in the community. These are referred to as health-care associated pneumonia (HCAP).
Pneumonia Pathogenesis:
The lungs are protected by many overlapping and redundant defense mechanisms. In the nose, hairs and turbinates collect larger particles and some organisms that would otherwise be inhaled from the environment. A key protective mechanism is the gag reflex and cough response are vital to prevent aspiration of gastric contents, ingested food and even saliva. Ironically, the resident population of bacteria in our oropharynx (normal flora) competes with pathogenic organisms and prevents colonization with more virulent bacteria.
Moving past the oropharynx and down into the airways, the principle mechanism protecting the lung is the mucociliary escalator. From the trachea down to some of the smallest branches, airway epithelium is covered in specialized ciliated and mucous producing cells. Because of the physics of flow, the velocity of air drops off rapidly as it is inhaled into the numerous smaller branches. Any particles in the inhaled air decelerate and literally drop onto the sticky layer of mucous produced by goblet cells. Cilia beat rhythmically raising this mucous toward the mouth and pharynx where it is swallowed. So then this epithelium is both a physical barrier and a removal system for any harmful substance that might enter our lungs. The epithelium also produces bacteriocidal peptides ("defensins") in the event inhaled bacteria want to infect and prey on lung tissue. Deep in the lungs where there is no ciliated epithelium, the smallest airways and alveoli are populated with alveolar macrophages that phagocytize bacteria then mount inflammatory and immune responses to any infective organism that makes it down to the "business end" of the airways.
When all of these defense mechanisms are overcome and the load of inhaled organisms exceeds the capacity of alveolar macrophages to eliminate them, pneumonia will develop. However, the symptoms of pneumonia are not caused directly by the bacteria growing in the lung tissue. Rather, the overwhelmed alveolar macrophages release inflammatory mediators (interleukins, tissue necrosis factors, and granulocyte colony-stimulating factor) which activate local and systemic responses. These include 1) fever, 2) rapidly rising WBC count and neutrophilia. Neutrophils that are attracted to the lung accumulate in the area of infected tissue and cause the build up of prurulent secretions. It is the production of these secretions that produce the rales (crackles) that are heard over an area of infected lung. The bacteria infecting the lung are thought to inhibit normal vasoconstrictive reflexes that typically shunt blood away from sick alveoli. Therefore, the patient's hypoxia can become relatively refractory.
Moving past the oropharynx and down into the airways, the principle mechanism protecting the lung is the mucociliary escalator. From the trachea down to some of the smallest branches, airway epithelium is covered in specialized ciliated and mucous producing cells. Because of the physics of flow, the velocity of air drops off rapidly as it is inhaled into the numerous smaller branches. Any particles in the inhaled air decelerate and literally drop onto the sticky layer of mucous produced by goblet cells. Cilia beat rhythmically raising this mucous toward the mouth and pharynx where it is swallowed. So then this epithelium is both a physical barrier and a removal system for any harmful substance that might enter our lungs. The epithelium also produces bacteriocidal peptides ("defensins") in the event inhaled bacteria want to infect and prey on lung tissue. Deep in the lungs where there is no ciliated epithelium, the smallest airways and alveoli are populated with alveolar macrophages that phagocytize bacteria then mount inflammatory and immune responses to any infective organism that makes it down to the "business end" of the airways.
When all of these defense mechanisms are overcome and the load of inhaled organisms exceeds the capacity of alveolar macrophages to eliminate them, pneumonia will develop. However, the symptoms of pneumonia are not caused directly by the bacteria growing in the lung tissue. Rather, the overwhelmed alveolar macrophages release inflammatory mediators (interleukins, tissue necrosis factors, and granulocyte colony-stimulating factor) which activate local and systemic responses. These include 1) fever, 2) rapidly rising WBC count and neutrophilia. Neutrophils that are attracted to the lung accumulate in the area of infected tissue and cause the build up of prurulent secretions. It is the production of these secretions that produce the rales (crackles) that are heard over an area of infected lung. The bacteria infecting the lung are thought to inhibit normal vasoconstrictive reflexes that typically shunt blood away from sick alveoli. Therefore, the patient's hypoxia can become relatively refractory.
This hypoxemia stimulates respiratory control centers which in turn drive up the respiratory rate (tachypnea) and depth. It is not unusual for patients with pneumonia to develop respiratory alkalosis as a result. Secretions that spill over into the airways stimulate sensory neurons, resulting in bronchospasm, cough, and air-hunger (dyspnea).
