Inflammation: A Fundamental Principle for Many Care Plans
The "innate" part of the immune system. Very primitive. Doesn't have to have seen the infecting particle previously. It just goes into action:
The body's inflammatory "tone" and immune competence are critical to understanding where on the health continuum your patient is located. Inflammation is a necessary prerequisite to healing. The ability to mount an inflammatory response to micro-organisms can limit and circumscribe the amount of damage an infection imposes upon the body. On the other hand, a poorly controlled inflammatory response can make cause sickness and tissue injury. Understanding the principles of the inflammatory response will strengthen your ability to assess your patient and articulate accurate problem statements.
The body's inflammatory "tone" and immune competence are critical to understanding where on the health continuum your patient is located. Inflammation is a necessary prerequisite to healing. The ability to mount an inflammatory response to micro-organisms can limit and circumscribe the amount of damage an infection imposes upon the body. On the other hand, a poorly controlled inflammatory response can make cause sickness and tissue injury. Understanding the principles of the inflammatory response will strengthen your ability to assess your patient and articulate accurate problem statements.
Inflammation and the "Castle Analogy"
Inflammation is a primitive, and early defense system. Humans are multi-cellular organisms constantly defending themselves against an environment that is loaded with bacteria, viruses, fungi, as well as particulate and toxins. Consequently, it's useful to compare it to a more easily grasped defense system... a medieval castle.
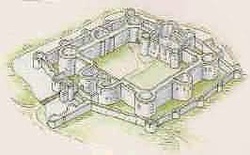
Note the general structure and layout of a castle: There were 2 types of people during the middle ages. Those that had stuff, and those that wanted to pillage stuff that belonged to others. So if you had stuff you'd try to build an impregnable fortress to protect it all. A lot of thought went into these structures. For instance:
1. They would be built on a hill so that those in the fortress could see the barbarians coming from a long way off and so that the had the "high ground" that was easier to defend, harder to attack.
2. The forests around a castle would be chopped down, again, to enhance the ability of the castle dwellers to spot anyone approaching with malign intentions.
3. The castle didn't just rely upon one set of stone walls. They almost always had (at least) two. And often, just to make successful attacks that much harder, they would surround the two walls with a moat full of water. (Hard to put a siege machine or a ladder against a wall if it was surrounded by water and muck.)
4. The tops of the defensive walls had crenelations on them that enabled defenders both a clear view and a defensive wall when needed.
1. They would be built on a hill so that those in the fortress could see the barbarians coming from a long way off and so that the had the "high ground" that was easier to defend, harder to attack.
2. The forests around a castle would be chopped down, again, to enhance the ability of the castle dwellers to spot anyone approaching with malign intentions.
3. The castle didn't just rely upon one set of stone walls. They almost always had (at least) two. And often, just to make successful attacks that much harder, they would surround the two walls with a moat full of water. (Hard to put a siege machine or a ladder against a wall if it was surrounded by water and muck.)
4. The tops of the defensive walls had crenelations on them that enabled defenders both a clear view and a defensive wall when needed.

Castles were structured to keep threats on the outside. Our bodies are also engineered to keep threats from the environment from entering. A castle wall was usually very thick, made of many layers of stone. In much the same way, our skin provides multiple layers of protection. There are at least 5 layers: (each one starts with the word "stratum").
1. Stratum basale, 2. spinosum, 3. granulosum, 4. licidum and finally 5. the stratum corneum. The names of the layers is barely relevant. But it's important to know that the deepest layer (basale) is where skin stem cells are found. It is here that new cells are generated after which they push themselves upward (or... the more top layers are worn away) and flatten as they go. And they die... so that by the time they reach the top (stratum corneum) they make up a flat, interlinking, no longer living, cornified layer of former cells. Their tight linkages provide a certain amount of water-proofing and are more or less impervious to larger particles and organisms. Where our bodies have no skin but still need protection, there is mucous membrane. (Lines the entire GI tract, the vagina, GU system, and the innermost layer of the airways)
1. Stratum basale, 2. spinosum, 3. granulosum, 4. licidum and finally 5. the stratum corneum. The names of the layers is barely relevant. But it's important to know that the deepest layer (basale) is where skin stem cells are found. It is here that new cells are generated after which they push themselves upward (or... the more top layers are worn away) and flatten as they go. And they die... so that by the time they reach the top (stratum corneum) they make up a flat, interlinking, no longer living, cornified layer of former cells. Their tight linkages provide a certain amount of water-proofing and are more or less impervious to larger particles and organisms. Where our bodies have no skin but still need protection, there is mucous membrane. (Lines the entire GI tract, the vagina, GU system, and the innermost layer of the airways)
A castle (no matter how well built) has to be actively defended!

There were always watchmen on the wall: You will recall (see above) all the steps that were taken to maximize visibility from high up on the castle walls. From this vantage point, watchmen could spot approaching enemy and if necessary, mount an initial defense. But the few archers/watchmen would never be enough to defend against a determined attack. Therefore, one of their most important roles was to sound the alarm, and notify the army of defenders within the castle that danger was present and a very robust defense was needed immediately!
The analogous cellular constituent in the body is the macrophage. Remember this point! Every tissue has it's own population of macrophages that are specialized to protect that tissue bed. The liver has Kupfer cells. The lung has the alveolar macrophage. And the macrophages in the brain are called microglia. Not only that... the intracellular fluid and spaces have roaming macrophages. But no matter where they end up, they all started in the same form, as monocytes in the bone marrow. These immature monocytes are released into the circulation where they float around until they find a tissue bed they like. They take up residence in that tissue or organ and undergo rapid change, adapting to their new environment. Like the watchmen on the castle walls, they are always on patrol, looking for anything irregular (suspicious). If they find trash that needs cleaning up, they phagocytize (eat) it, digest it and finally "burp out" the remaining elements that can be absorbed into the body system.
Certainly, in medieval times, it was important for the defenders of the castle to NOT go around killing rightful inhabitants that lived within the fortress! That's why they all wore some sort of "livery" or uniform, so the castle population could be identified and left alone. In much the same way, there are "ID tags" on each cell of the body that reassure the resident macrophages, telling them to refrain from attacking "self" cells.
As noted above, the most important thing the watchmen did was to alert the major defenders of the castle when danger was present, while at the same time, mounting an initial defense. Macrophages do much the same thing. Their initial efforts at defending against (for example) bacteria would be to phagocytize the infecting organisms. But immediately after they ingest a few invading cells, the macrophages begin releasing chemical signals (chemokines, interleukins, tissue necrosis factors) that serve as powerful activators of and attractants of other cells to the site of the "invasion." This movement to the site of the infection is called "chemotaxis". The chemical signals released by the macrophages don't just call forth the "army" of leukocyte defenders. They also rev up the macrophage itself (this is called "autocrine" signaling). Under these conditions, the macrophage becomes a more effective killer.
The analogous cellular constituent in the body is the macrophage. Remember this point! Every tissue has it's own population of macrophages that are specialized to protect that tissue bed. The liver has Kupfer cells. The lung has the alveolar macrophage. And the macrophages in the brain are called microglia. Not only that... the intracellular fluid and spaces have roaming macrophages. But no matter where they end up, they all started in the same form, as monocytes in the bone marrow. These immature monocytes are released into the circulation where they float around until they find a tissue bed they like. They take up residence in that tissue or organ and undergo rapid change, adapting to their new environment. Like the watchmen on the castle walls, they are always on patrol, looking for anything irregular (suspicious). If they find trash that needs cleaning up, they phagocytize (eat) it, digest it and finally "burp out" the remaining elements that can be absorbed into the body system.
Certainly, in medieval times, it was important for the defenders of the castle to NOT go around killing rightful inhabitants that lived within the fortress! That's why they all wore some sort of "livery" or uniform, so the castle population could be identified and left alone. In much the same way, there are "ID tags" on each cell of the body that reassure the resident macrophages, telling them to refrain from attacking "self" cells.
As noted above, the most important thing the watchmen did was to alert the major defenders of the castle when danger was present, while at the same time, mounting an initial defense. Macrophages do much the same thing. Their initial efforts at defending against (for example) bacteria would be to phagocytize the infecting organisms. But immediately after they ingest a few invading cells, the macrophages begin releasing chemical signals (chemokines, interleukins, tissue necrosis factors) that serve as powerful activators of and attractants of other cells to the site of the "invasion." This movement to the site of the infection is called "chemotaxis". The chemical signals released by the macrophages don't just call forth the "army" of leukocyte defenders. They also rev up the macrophage itself (this is called "autocrine" signaling). Under these conditions, the macrophage becomes a more effective killer.
The "Shock Troops"

In medieval times, the most elite troops were the mounted knights: Imagine how thrilling it would be to see a charge or horse-mounted knights. Alerted by the watchmen on the castle wall that there was an enemy advancing upon the fortress, the elite knights would mount up, charge forth, and attempt to annihilate the attackers. That would be neat to see. Now imagine you're a peasant whose humble farm, cottage, and pastures happened to be "in the way" of the cavalry charge. Certainly, the troops of mounted knights were the most effective, and the most feared warriors of their day. But they were also (sad to say) rather indiscriminate killers as well. There was what we would call today, a lot of "collateral damage".
The cellular counterpart to the army of mounted knights is the neutrophil: In the event of an infection, when macrophages have phagocytized some organisms and released chemical signals, the bone marrow releases millions of neutrophils, which are then brought to the site of the infection by the chemokines released by the macrophages (remember, this is chemotaxis). Another thing that these chemical mediators do, is to prepare the "battlefield" so that when the neutrophils arrive, they can get out to the infected or injured area and exit the circulation to enter the wound.
The cellular counterpart to the army of mounted knights is the neutrophil: In the event of an infection, when macrophages have phagocytized some organisms and released chemical signals, the bone marrow releases millions of neutrophils, which are then brought to the site of the infection by the chemokines released by the macrophages (remember, this is chemotaxis). Another thing that these chemical mediators do, is to prepare the "battlefield" so that when the neutrophils arrive, they can get out to the infected or injured area and exit the circulation to enter the wound.
The most abundant cell in pus is the neutrophil
What does an infected wound look like? Well, it's red, warm, swollen, painful and generally, the wounded part doesn't work so well. The redness, warmth and swelling of an inflamed tissue are due to the action of cytokines and chemical mediators. The capillary beds of the wound dilate (resulting in warmth and redness), and they become "leaky", releasing fluid into the intracellular spaces of the wounded tissues (swelling.) All of these actions help neutrophils get to where they need to be. As stated above, given the right soup of chemical mediators, the bone marrow begins to release millions and millions of neutrophils. These circulate throughout the body until they get to the "battlefield." At that point, the neutrophils get sticky and adhere to the capillary walls. (This is called "margination".) Because the capillaries are already leaky, the neutrophils squeeze through the small blood vessel walls. (This is called "diapedesis") At LAST!!! They are where the action is and they begin fighting the infection with a number of powerful molecular weapons. (But... sadly, those weapons also injure any nearby cell or tissue.) Specifically, neutrophils are phagocytes. Therefore they begin to ingest bacteria. They also empty out intracellular granuoles that contain proteins that ensnare bacteria. But mostly they release chemicals that kill bacteria. Some of these chemicals are enzymes, others are powerful oxidizing agents. They are toxic to bacteria and "self" cells as well.
Clinical labs:

When your patient has, or is suspected to have, an infection, one of the labs that will be ordered is a CBC (Complete Blood Count). Naturally, the CBC will provide essential information like the patient's hematocrit (Hct) and hemoglobin (Hgb), erythrocyte count, and description of the erythrocytes' appearance (size and color.) But for the purpose of evaluating the patient for infection, the white blood cell (WBC) count is the most vital. Under normal conditions, the WBC count ranges roughly between 5000 and 10,000. (Different labs and texts have slightly different ranges.) Neutrophils are usually the most abundant cell in the WBC count and it's reported as a %. The normal percentage of neutrophils is (again, depending upon the reference you read) between 50 and 70%. When a patient has an infection (particularly a bacterial infection) the WBC count will rise precipitously. (This is called "neutrophilia") Also the % of neutrophils will increase. There is one other thing that the CBC may report. As stated earlier, when stimulated by cytokines and other chemical mediators, the bone marrow will literally "erupt" in neutrophil release. These are neutrophils that are just waiting for their turn to enter the circulation. Suppose the infection is very, very, very severe. The bone marrow will run out of mature neutrophils and will begin to spit out "baby" neutrophils. An adult neutrophil has a segmented nucleus. Just to confuse students, this one cell type has many names. 1) neutrophil 2) polymorphonucleated lymphocyte ("polys" or "PMLs") and 3) segs (i.e., segmented nucleus.) An immature neutrophil has a non-segmented nucleus. Normally only 3-7% of the WBC is immature. But when the infection is severe, the % will rise. These cells also (just to confuse students) go by different names. They are sometimes called "bands" and sometimes called "stabs".
Have you ever heard someone say a patient has a "left shift"? A "left shift" is a high WBC count, an increased % of neutrophils, and (sometimes) the appearance of more than a normal amount of bands (or stabs). A left shift in your patient's CBC is strongly suggestive of a bacterial infection.
Have you ever heard someone say a patient has a "left shift"? A "left shift" is a high WBC count, an increased % of neutrophils, and (sometimes) the appearance of more than a normal amount of bands (or stabs). A left shift in your patient's CBC is strongly suggestive of a bacterial infection.
Parenthetically:
The other half of the immune system is called "acquired immunity". It involves T and B cells and the production of antibodies. The tissue macrophage plays an important role in activating this process. But acquired immunity can wait. We aren't discussing it now.
