Refractory Hypoxemia:
Deoxygenated blood returns to the heart from the periphery goes through the right atrium, out through the pulmonary artery (the only artery in the body that is NOT supposed to carry richly oxygenated blood.)
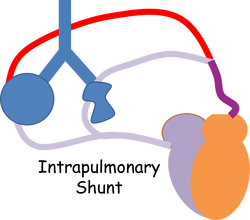
Try to imagine this blood as individual red blood cells. What you must understand is that RBC's don't wander around the lungs sipping O2 from lots of alveoli. Rather, each RBC is going to have 1 (only one) shot at picking up oxygen... they will only see one alveolus before they head back to the left side of the heart. The RBC that goes past the nice round alveolus in the picture, returns to the heart oxygenated. The RBC that visits the shriveled up alveolus (collapsed due to pneumonia and filled with exudate) will return to the heart just like it left... with hardly any oxygen added to its hemoglobin. Both of these RBC's (the one that got lucky and the one that didn't) will join each other in the pulmonary vein (the only vein in the body intended to carry oxygenated blood.) There they mix.
So far we've made some sense out of why Mr. G. is hypoxic and why the blood going to his body will be less oxygenated. But what does "refractory" mean? Look at the picture. Suppose this patient (Mr. G) is now breathing a high concentration of oxygen. The "lucky" RBC might pick up a little more O2 on its hemoglobin. But nothing (nada, nyet, zilch, zero) will help the RBC that visited the shriveled alveolus. So no matter how much oxygen the patient is breathing, deoxygenated blood will still be dumped into the left side of his heart and pumped out to his body.
Another term that is applied to this phenomenon is V/Q mismatch. (V = ventilation, Q = perfusion) (and I have no idea why it's "Q" except that "P" which makes more sense is usually used to mean "pressure".
Try to imagine this blood as individual red blood cells. What you must understand is that RBC's don't wander around the lungs sipping O2 from lots of alveoli. Rather, each RBC is going to have 1 (only one) shot at picking up oxygen... they will only see one alveolus before they head back to the left side of the heart. The RBC that goes past the nice round alveolus in the picture, returns to the heart oxygenated. The RBC that visits the shriveled up alveolus (collapsed due to pneumonia and filled with exudate) will return to the heart just like it left... with hardly any oxygen added to its hemoglobin. Both of these RBC's (the one that got lucky and the one that didn't) will join each other in the pulmonary vein (the only vein in the body intended to carry oxygenated blood.) There they mix.
So far we've made some sense out of why Mr. G. is hypoxic and why the blood going to his body will be less oxygenated. But what does "refractory" mean? Look at the picture. Suppose this patient (Mr. G) is now breathing a high concentration of oxygen. The "lucky" RBC might pick up a little more O2 on its hemoglobin. But nothing (nada, nyet, zilch, zero) will help the RBC that visited the shriveled alveolus. So no matter how much oxygen the patient is breathing, deoxygenated blood will still be dumped into the left side of his heart and pumped out to his body.
Another term that is applied to this phenomenon is V/Q mismatch. (V = ventilation, Q = perfusion) (and I have no idea why it's "Q" except that "P" which makes more sense is usually used to mean "pressure".
