Carefully read through this CRT. Then look through the pathophysiology discussed below.
With an understanding of DKA pathophysiology you should be able to critique this CRT. 1. Are all the assessments "focused"? That is, do they relate to the problem with which they are associated? 2. Are the problem statements in order from most to least urgent? Are they articulated in 3 parts? (Problem statement, RT, Cause of problem, AEB, symptoms that cinch the deal and support your problem statement.) 3. Do the goals specifically relate to the problem statement with which they are associated? Are they written in a time context? Are they measureable (or binary... yes/no)? And are they reasonable? 4. The nursing actions (just like the rest of your clinical reasoning) should relate to the problem with which they are associated. Ideally, written as nursing "orders" (imperative verb form) not suggestions. They describe the means and methods of accomplishing the action. 5. The evaluation relates to the goal statement and explains if the goal was met (hooray!) or not (back to the drawing board.)

Mr. V. is a 24 year old non-English speaking, undocumented immigrant who has been working as a day-laborer for the past 6 months and living with his cousin's family in a crowded apartment. Over the last several weeks he has become increasingly fatigued, unable to work, lost his appetite, and dropped 8 pounds. It seems all he's had time to do is drink and pee. Finally his cousin's wife became alarmed because he was also throwing up and seemed sometimes to not be making a lot of sense. Fear of discovery may have delayed Mr. V. from getting care until his symptoms were quite advanced. He arrived with his family in the emergency room at about 1:30 AM.
Observations: Mr. V. is a thin but well-developed young man lying semi-recumbent on a gurney. He is very lethargic, though he can be aroused. He has had one episode of vomiting clear stomach contents since he arrived. His skin is warm, dry and flushed. The emergency room nurse notices that there are ketones on Mr. V's breath.
Vital signs: T 96.8, P 128, R 28 and very deep and labored (Kussmal breathing.) BP 102/48, %sat 100 on room air.
Examination: Unfortunately the nurse does not speak Spanish and the gathered family's cumulative English is limited. The house supervisor is notified that a medical translator is needed as soon as one is available. Because of the language barrier, it is difficult to know how oriented Mr. V. is and how well he follows commands. Consequently assessing Mr V's level of consciousness is somewhat inexact. Mr. V's pupils however are 3 mm and PERRL, appear to be tracking normally without extraocular movements. He moves all extremities equally. The nurse notices that while lying at a 45 degree angle, Mr. V. does not have any jugular vein distension. Auscultation of his chest finds clear breath sounds and a normal (but tachycardic) S1 and S2. His bowel sounds are normoactive. The nurse cannot get a clear answer to questions about Mr. V's bowel habits. Mr. V. however is using the urinal and voiding 280 ml straw colored urine. The nurse finds 1-2+ pulses in all extremities and sluggish capillary refill.
Labs:
Chemistries: Na+ 133, K+ 4.0, Cl- 109, HCO3- 10, BUN 35, Creatinine 1.9, Glucose 733
Heme: Hgb 18, Hct 52, WBC 15,000, platelets 390,000
ABG's: PaO2 90, PaCO2 20, pH 7.26 %sat 100 on room air.
CXR was read as normal
EKG: Sinus tachycardia with ST segment depression, prolonged QT interval
UA: 4+ ketones
Observations: Mr. V. is a thin but well-developed young man lying semi-recumbent on a gurney. He is very lethargic, though he can be aroused. He has had one episode of vomiting clear stomach contents since he arrived. His skin is warm, dry and flushed. The emergency room nurse notices that there are ketones on Mr. V's breath.
Vital signs: T 96.8, P 128, R 28 and very deep and labored (Kussmal breathing.) BP 102/48, %sat 100 on room air.
Examination: Unfortunately the nurse does not speak Spanish and the gathered family's cumulative English is limited. The house supervisor is notified that a medical translator is needed as soon as one is available. Because of the language barrier, it is difficult to know how oriented Mr. V. is and how well he follows commands. Consequently assessing Mr V's level of consciousness is somewhat inexact. Mr. V's pupils however are 3 mm and PERRL, appear to be tracking normally without extraocular movements. He moves all extremities equally. The nurse notices that while lying at a 45 degree angle, Mr. V. does not have any jugular vein distension. Auscultation of his chest finds clear breath sounds and a normal (but tachycardic) S1 and S2. His bowel sounds are normoactive. The nurse cannot get a clear answer to questions about Mr. V's bowel habits. Mr. V. however is using the urinal and voiding 280 ml straw colored urine. The nurse finds 1-2+ pulses in all extremities and sluggish capillary refill.
Labs:
Chemistries: Na+ 133, K+ 4.0, Cl- 109, HCO3- 10, BUN 35, Creatinine 1.9, Glucose 733
Heme: Hgb 18, Hct 52, WBC 15,000, platelets 390,000
ABG's: PaO2 90, PaCO2 20, pH 7.26 %sat 100 on room air.
CXR was read as normal
EKG: Sinus tachycardia with ST segment depression, prolonged QT interval
UA: 4+ ketones
Clinical Reasoning about Mr. V.
Oxygenation:
It would be a difficult task to demonstrate any oxygenation problem Mr. V. could have unless you noted that his heart was beating very fast and had some non-specific EKG changes. However, he is young, male and otherwise fit. Mr. V's heart is beating very fast because he is severely dehydrated and his heart has to work harder to recycle blood throughout the body. But we will deal with this below.
Fluid and Electrolytes/Acid-Base balance: Mr. V. has several threats to this most basic of basic human needs. We'll address them one at a time:
1. Hypovolemia: When Mr. V's beta cells stopped making insulin, several things happened. Obviously glucose was not being transported into cells. This sets into motion several counter-regulatory processes that make glucose concentration increase as well. The body secretes more glucagon, cortisol, epinephrine and growth hormone.. All of these events promot actions in the liver that result in gluconeogenesis, glycogenolysis and lipolysis. Taken together these events produce a massive increase in circulating glucose. The breakdown of free fatty acids, meanwhile, results in formation of ketoacids. The renal threshold for glucse is around 180 mg/dL. Mr. V. has been exceeding that for sometime now and a lot of glucose has spilled into the tubular (kidney) filtrate. This has caused an osmotic diuresis and even though Mr. V. has been drinking as much as he could, he has not been keeping up. (This hasn't been helped any by the fact that the build up of ketones causes nausea and vomiting.) Observations such as his tachycardia and low blood pressure also support the suggestion that Mr. V. is dehydrated.
2. Hyperosmolarity: If you have been paying very close attention, you'll notice that many of Mr. V's lab values support your hunch that the patient is hypovolemic. That is, his BUN and Creatinine are very elevated. But typically a dehydrated patient should have a high serum sodium as well... and he doesn't. Why would that be? As Mr. V's blood glucose has been rising, his blood has become hyperosmolar ("thick" if you will, the way syrup is thicker than water), which will trigger several compensatory mechanisms. This hyperosmolarity will be sensed in the hypothalamus leading to the release of ADH which will promote water reabsorption. (But this probably won't work too well... remember the patient is having an osmotic diuresis. ADH cannot fix that.) But, other hormones (aldosterone for example) will act upon the distal tubule of the nephron to cause it to dump sodium. So as the glucose concentration goes up, Mr. V's body will try to compensate and maintain osmolar balance with the result that serum sodium levels fall.
3. Hypokalemia: Mr. V. is going to have postassium derangement for several reasons. First of all, there is a certain amount of "obligatory" potassium loss in the urine at all times, especially when there is a lot of urine being produced. You will recall that Mr. V's condition has been associated with nausea and vomiting. He has not replaced the potassium he's been throwing up and loosing in his urine. The second reason he's at risk for hypokalemia is...
It would be a difficult task to demonstrate any oxygenation problem Mr. V. could have unless you noted that his heart was beating very fast and had some non-specific EKG changes. However, he is young, male and otherwise fit. Mr. V's heart is beating very fast because he is severely dehydrated and his heart has to work harder to recycle blood throughout the body. But we will deal with this below.
Fluid and Electrolytes/Acid-Base balance: Mr. V. has several threats to this most basic of basic human needs. We'll address them one at a time:
1. Hypovolemia: When Mr. V's beta cells stopped making insulin, several things happened. Obviously glucose was not being transported into cells. This sets into motion several counter-regulatory processes that make glucose concentration increase as well. The body secretes more glucagon, cortisol, epinephrine and growth hormone.. All of these events promot actions in the liver that result in gluconeogenesis, glycogenolysis and lipolysis. Taken together these events produce a massive increase in circulating glucose. The breakdown of free fatty acids, meanwhile, results in formation of ketoacids. The renal threshold for glucse is around 180 mg/dL. Mr. V. has been exceeding that for sometime now and a lot of glucose has spilled into the tubular (kidney) filtrate. This has caused an osmotic diuresis and even though Mr. V. has been drinking as much as he could, he has not been keeping up. (This hasn't been helped any by the fact that the build up of ketones causes nausea and vomiting.) Observations such as his tachycardia and low blood pressure also support the suggestion that Mr. V. is dehydrated.
2. Hyperosmolarity: If you have been paying very close attention, you'll notice that many of Mr. V's lab values support your hunch that the patient is hypovolemic. That is, his BUN and Creatinine are very elevated. But typically a dehydrated patient should have a high serum sodium as well... and he doesn't. Why would that be? As Mr. V's blood glucose has been rising, his blood has become hyperosmolar ("thick" if you will, the way syrup is thicker than water), which will trigger several compensatory mechanisms. This hyperosmolarity will be sensed in the hypothalamus leading to the release of ADH which will promote water reabsorption. (But this probably won't work too well... remember the patient is having an osmotic diuresis. ADH cannot fix that.) But, other hormones (aldosterone for example) will act upon the distal tubule of the nephron to cause it to dump sodium. So as the glucose concentration goes up, Mr. V's body will try to compensate and maintain osmolar balance with the result that serum sodium levels fall.
3. Hypokalemia: Mr. V. is going to have postassium derangement for several reasons. First of all, there is a certain amount of "obligatory" potassium loss in the urine at all times, especially when there is a lot of urine being produced. You will recall that Mr. V's condition has been associated with nausea and vomiting. He has not replaced the potassium he's been throwing up and loosing in his urine. The second reason he's at risk for hypokalemia is...
Remember...
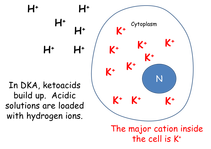
...most of the body's potassium is intracellular. While Mr. V. has been getting increasingly ketoacidotic, hydrogen ions have been building up in his extracellular fluids.
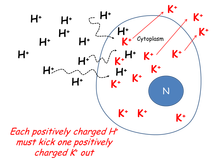
Because there is an increase of hydrogen ions on one side of the cell wall, some of them will diffuse down their concentration gradient and enter the cell. This is a problem. If a positively charged ion moves into the cell, a positively charged ion must leave. Since the most abundant intracellular cation is potassium... potassium ions will begin to exit the cell and get into the extracellular fluid.
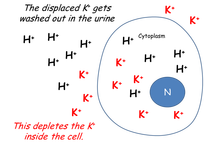
Don't forget... whenever the body is making urine, there is going to be an "obligatory" potassium loss. All of these potassium ions leaving the interior of cells are getting washed away in the urine. Therefore, the body is getting seriously potassium depleted!
But wait a minute! When we looked at Mr. V's serum chemistries, his potassium looked OK?!!! (It was 4.0 which is just fine... normally.) The reason for this seeming contradiction is that this is a dynamic process. K+ is being continuously "driven" out of the cells by the hydrogen ions entering them.
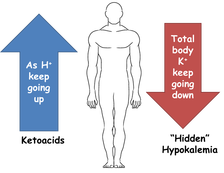
So what's the big deal? Well... suppose we are very successful at reversing Mr. V's DKA (by giving him insulin). That would mean he would stop making ketoacids and the pH of his body fluids (which is very low) would begin to rise toward normal. This means that the concentration of hydrogen ions in the extracellular fluid will go down. This also means that hydrogen ions will exit the cell. BUT for every positively charged hydrogen ion that leaves the interior of the cell, a potassium ion must enter to take its place. That means the extracellular potassium concentration will begin to crater. Mr. V. could conceivably quickly die of hypokalemia if he were given insulin unwisely.
So what's the big deal? Well... suppose we are very successful at reversing Mr. V's DKA (by giving him insulin). That would mean he would stop making ketoacids and the pH of his body fluids (which is very low) would begin to rise toward normal. This means that the concentration of hydrogen ions in the extracellular fluid will go down. This also means that hydrogen ions will exit the cell. BUT for every positively charged hydrogen ion that leaves the interior of the cell, a potassium ion must enter to take its place. That means the extracellular potassium concentration will begin to crater. Mr. V. could conceivably quickly die of hypokalemia if he were given insulin unwisely.
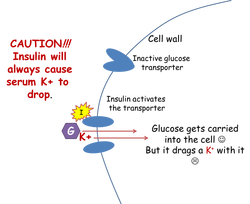
But wait!!! There is a third reason Mr. V. is in danger of suffering a serious, life-threatening drop in his serum K+. In order to reverse his DKA, he will need insulin, which will transport glucose into the cell. Once it is in the cell, Mr. V no longer needs to generate energy from fatty acids (that produce ketones as a by-product.)
Hooray!
Oh, NO!
There is one more problem, however. When insulin molecules turn "ON" the glucose transporters, glucose will enter the cell (good) but will drag potassium with it. (Bad.)
Hooray!
Oh, NO!
There is one more problem, however. When insulin molecules turn "ON" the glucose transporters, glucose will enter the cell (good) but will drag potassium with it. (Bad.)
Nutrition: Mr. V. has been starving ever since his insulin producing Beta cells petered out on him. That is to say, muscle and fat cells have been without their normal fuel (glucose). The mitochondria in these cells have had to generate ATP by burning fatty acids (and of course producing ketoacids that we've already discussed. They have also used up a lot of intracellular phosphate to accomplish that task. Additionally, during acidotic conditions, phosphate (like potassium) tends to leave the intracellular fluid and move into extracellular fluid and eventually is wasted in urine. Consequently, Mr. V's total body phosphate stores are unbalanced.
Elimination: At this point we have no reason to believe that Mr. V's urinary system and bowels are not working just fine.
Rest and Recovery: Mr. V. is extremely fatigued and debilitated. He's experiencing nausea and throwing up. He probably has not rested well in days and days. Sometimes patients with DKA will have chest pain and/or arthralgias. However, he has not reported any pain and unless he says something to the contrary, there is no reason to treat any pain.
Mobility: Mr. V. has been a healthy young man up to this point. He is now weak and fatigued. Though DKA would not ordinarily impair mobility, the debility might. He should be on bed rest and have assistance if he needs to get out of bed.
Physiological Safety: 1. Functioning cortex: You will recall that Mr. V. has been living with some extended family and that the precipitating event that caused them to bring him to the hospital was his change in level of consciousness. In fact, the hyperosmolar state characteristic of DKA has profound effects upon brain cells. For that reason, Mr. V's neurological status should be monitored closely. 2: Immune system: Infection and the associated cytokines and cortisol (stress hormone) production can precipitate hyperglycemia and cause even normally well-controlled diabetics to become very brittle. For this reason the clinician should be alert to the possibility that Mr. V. has a sub-clinical infection at this time. However, in DKA, an elevated white count could be a nonspecific stress response, and not necessarily an infection. The fact that he is afebrile supports this supposition.
Elimination: At this point we have no reason to believe that Mr. V's urinary system and bowels are not working just fine.
Rest and Recovery: Mr. V. is extremely fatigued and debilitated. He's experiencing nausea and throwing up. He probably has not rested well in days and days. Sometimes patients with DKA will have chest pain and/or arthralgias. However, he has not reported any pain and unless he says something to the contrary, there is no reason to treat any pain.
Mobility: Mr. V. has been a healthy young man up to this point. He is now weak and fatigued. Though DKA would not ordinarily impair mobility, the debility might. He should be on bed rest and have assistance if he needs to get out of bed.
Physiological Safety: 1. Functioning cortex: You will recall that Mr. V. has been living with some extended family and that the precipitating event that caused them to bring him to the hospital was his change in level of consciousness. In fact, the hyperosmolar state characteristic of DKA has profound effects upon brain cells. For that reason, Mr. V's neurological status should be monitored closely. 2: Immune system: Infection and the associated cytokines and cortisol (stress hormone) production can precipitate hyperglycemia and cause even normally well-controlled diabetics to become very brittle. For this reason the clinician should be alert to the possibility that Mr. V. has a sub-clinical infection at this time. However, in DKA, an elevated white count could be a nonspecific stress response, and not necessarily an infection. The fact that he is afebrile supports this supposition.
3. Clotting Cascade: There are reports in the literature about children with DKA having strokes, and reports that link DKA with DIC. At this moment we have no assessment data to suggest that Mr. V. is experiencing any coagulopathy
Higher Order Needs.
The tragic thing about Mr. V's situation is that he has some severe problems within Maslow's "second story" hierarchical level. This is a level devoted to "Safety"... but not physiological safety. The needs in Maslow's second story have to do with situational safety. In order to be situationally safe, Mr. V. must have access (at minimum!) to the knowledge necessary to manage his diabetes and the tools (insulin, glucometer, test-strips) to do so. His lack of resources and fear of discovery may precipitate a repeat episode of ketoacidosis, or the long-term complications of chronic hyperglycemia (renal failure, blindness, peripheral vascular disease, neuropathy.) The nurse has thought about these issues and included them in the plan of care. Is it enough for Mr. V? It's a start.
