Asthma Pathophysiology:
Asthma is an episodic, somewhat reversible episode of airway obstruction. It is characterized by (1) "twitchy airways" (hyper-responsiveness of airway smooth muscle), (2) edema and inflammation of the airway mucosa, and (3) production of thick, abnormal sputum which taken together produce airway obstruction. In poorly reversible asthma that sometimes "simmers" in a subacute or chronic state of inflammation, airways are "remodeled" and airway obstruction becomes increasingly chronic. This state is promoted by invasion of the tissues with eosinophils and monocytes. These cells (and other participants such as sensory nerve fibers and mast cells) produce a cytokine/chemical mediator "soup" that results in loss of normal ciliated epithelial cells that usually populate the mucosa, and hyperplasia of airway smooth muscle and promote permanent changes
The clinical hallmarks of asthma include dyspnea and tachypnea, cough (sometimes productive, often not), wheezing (though sometimes not present) and complaints of chest tightness or pain. Most importantly, during an episode of asthma, the mechanics of breathing are distorted, producing an increase in the work of breathing, hypoxia and (in severe cases resulting in respiratory failure) hypercapnea. To understand how even small changes in the diameter of airways influences breathing, consider the architecture of the respiratory tree.

Look at the numbers on the right side of this table. You can see that as the branches become smaller and smaller, they become massively more numerous. You might be asking yourself "isn't it harder to get air through narrow little airways? Isn't there a high resistance to flow?" (We know what happens when the nozzle on a hose narrows the outflow of water... But no that's not what happens in the lung.) Think of one miniscule airway. It WOULD take a lot of pressure to push air through it. 2 miniscule airways would require half as much pressure. 4 miniscule airways would take maybe half as much pressure than it took to blow air through 2. Carry that logic out to about a bazillion small airways and you can see why airflow into and out of the lung is supposed to be such a low pressure operation.
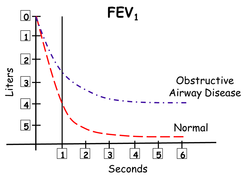
The consequences of these adverse changes can be seen in the diagram to the left. Under normal conditions an individual can take in a maximal breath, and within 1 second blow most of it out (red line). This becomes impossible when patients have airway obstruction. During an attack of asthma, the obstruction so interferes with the exit of air from the lungs, that the patient initiates the next breath before the preceding one is completely exhaled. Gradually, during the course of the episode, a condition called dynamic hyperinflation begins to occur. The air in the lung at the end of a breath is referred to as the functional residual capacity (FRC). It is obvious then that the patient with airway obstruction begins to have a gradual increase in FRC. This means they must initiate the next breath at a much higher lung volume and to do so must generate more negative pressure in the chest. To make this situation worse, a hyperinflated lung presses down upon and flattens the diaphragm making it less effective in inspiration. Thus, an actively asthmatic patient must utilize the accessory muscles of respiration (trapezius, sternclaidomastoid) to breathe in. Another adaptation to the increased work of breathing is that the expiratory phase of the respiratory cycle is no longer passive. The patient must use their abdominal and intercostal muscles to exhale.
Changes in diffusion of respiratory gasses during asthma episodes:
It should be remembered that oxygen diffuses 20 times less readily than carbon dioxide. Not surprisingly, then, the first evidence of impaired gas exchange during an acute bout of airway obstruction is hypoxemia. In addition, the relationship between ventilation and perfusion becomes mismatched in areas of the lung causing refractory hypoxia.
Counter-intuitively, however, early on in an asthma attack, the concentration of carbon dioxide in blood will actually be reduced. This is for (at least) 2 reasons. First, as already stated, carbon dioxide diffuses very readily. Second, because the patient is beginning to become hypoxic, the respiratory control centers in the medulla drive respiratory effort.
A 16 year old with Life-Threatening Asthma

Back story: CG is 16 years old and has been a poorly controlled asthmatic since 3 years of age. She is supposed to be on a lot of medications including (1) Advair inhaler (2) Albuterol inhaler (3) Theo-dur tablets (4) Prednisone (5) Accolate (6) Intal inhaler. That's a lot of medications to keep straight. And (not to be redundant) she is a teenager and non-compliant. Theo-dur makes her "shaky" and prednisone makes her "fat and gives me zits". Not only that, she got the idea that most of her inhalers could be used for rescue purposes. And not only that... she really hates the hospital and has waited way too long to admit to herself that she needs help NOW. The faculty adviser at the cheer-leading try-outs saw that CG was in distress and called the paramedics. CG is in the ER and the health-care team is trying to keep her out of the ICU and off a ventilator.
Let's talk about the significance of each part of the nurse's clinical reasoning table
Brief background: This section only includes who, why and how long. It's sketchy and limited for 2 reasons. First: This is really the best way to give report (or hand-off or SBAR). It immediately orients the other team members to the basic facts and puts the rest of report into a context. Report should never be a stream-of-consciousness narrative. So start with who, why and how long. Second: If there is other information that is genuinely important, guess what? It should be part of your assessment!
Focused Assessment: This part of the nursing process should contain all of the significant data (for each problem) and nothing extraneous. Does the focused assessment here meet that criteria? Check it out.
1. "Last admit for respiratory failure 6 months ago!" This is an example of background history that has direct significance to this particular problem. It rightfully is assessment and not general background information
Focused Assessment: This part of the nursing process should contain all of the significant data (for each problem) and nothing extraneous. Does the focused assessment here meet that criteria? Check it out.
1. "Last admit for respiratory failure 6 months ago!" This is an example of background history that has direct significance to this particular problem. It rightfully is assessment and not general background information
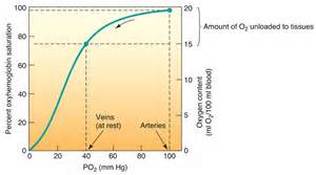
2. Vitals signs immediately indicate the patient is very sick in particular her tachycardia, tachypnea, and refractory hypoxia. (Time out. What is "refractory hypoxia". "Refractory" means resistant to change. If a normal person is on 3 liters/min of oxygen, their %sat would be 100. In spite of being on a high concentration of inhaled oxygen, CG is only at 88%. She is slipping over the "shoulder" of the oxyhemoglobin dissociation curve... meaning small decreases in oxygenation at this point profoundly reduce the diffusing pressure of oxygen in her serum. In other words, she will be oxygenating her tissues poorly. Taken together the vital signs tell the nurse this patient is in big trouble. Some team member is going to crank up the O2 right away. Will it work? Only a little.
3. Observations: The first thing a nurse should when caring for an acutely ill person (especially one with respiratory difficulty) is to look at the patient critically. This patient is sitting upright (you wouldn't be able to get her to lie down no matter what you did) because, among other things, she has hyperinflated lungs and she would feel smothered if her abdominal contents were pressing against her diaphragm. She is in tripod position to make it easier for her to recruit the accessory muscles of respiration (like the trapezius and sternoclaidomastoid.) This is necessary for a patient with hyperinflated lungs... These muscles lift the chest wall out and up. She has to use these extreme measures just to move a little fresh air into her lungs. Exhalation is almost always passive. The use of abdominal muscles (in a resting patient) to breathe out always means airway resistance. It is almost the sine qua non of airway obstruction. CG is coughing because her airways are inflamed and irritated by a soup of chemical mediators. But she can't move air fast enough for her cough to be effective.
