A Clinical Reasoning Table for Mrs. R.
Focused Assessment: As has been stated previously, focused assessments are those that relate to the problem statement. Extraneous data is left out so as to not clutter up reasoning. There quite a few problems associated with Mrs. R's condition and they may all overlap. Consequently the assessment column may seem less streamlined than those for other sample patients. Some of the issues present us a "chicken and egg" question. Did Mrs. R get a UTI which caused her to be less cognitively aware and therefore less likely to drink and stay hydrated? Or, did some event cause her to drink less, which caused the UTI and the change in mental status?
Because these factors are so inter-related, the assessments are just listed in an arbitrary order in the first column. Nevertheless, there is no extraneous information present. There is sufficient information to demonstrate Mrs. R has a problem with fluid imbalance, nutrition, and two problems related to physiological safety, infection and a diminished sensorium.
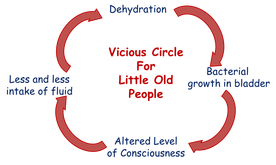
Problem Statements: In an "epistemic" approach to clinical reasoning there are not hundreds of diagnoses. Rather, there is a finite set of basic human needs, any of which can be either threatened or actually impaired. Because they are listed in order of urgency, Fluid/Electrolyte needs lead the list. Mrs. R. is dehydrated. It should be noted that the nurse does not need to know everything about Mrs. R. in order to write the diagnosis. Since the nurse doesn't know (who does?) what caused her to fail this way, a "place-holder" cause is mentioned after "RT". The nurse speculates that Mrs. R stopped drinking adequate amounts of fluids. It is not necessary to know why she might have done so at this point. (See "Vicious Circle" above.) The evidence cited after "AEB" is enough to support the diagnosis but does not double the work by requiring the nurse or student to rewrite all the assessments in the problem statement. Either a summary of them, or a few key assessments is reasonable. Students note: This is the most common type of dehydration (hypernatremic, hypovolemic). The classic hallmarks are elevated sodium, BUN and Creatinine, hemoglobin and hematocrit. Therefore, when you are assessing a patients hydration you must note these 3 values on their basic metabolic panel and at lease 2 on the heme studies.
The remainder of the problem statements are listed in an order the nurse judges to be correct. In this situation the nurse has listed the infection as second in urgency. It is, (based upon the CBC) an acute infection and Mrs. R needs to have her antibiotics started ASAP.
The third problem statement is listed as impaired nutrition. Physiologically a more urgent need than "Safety", but it is obviously a chronic problem. It did not develop within the last few days.
The fourth problem is impaired safety related to Mrs. R's depressed sensorium. If this is "metabolic" in origin, it will clear as the other needs (fluid, infection control and nutrition) are resolved. The nurse does not know what Mrs.R's best baseline mentation is and clearly indicates that some parts of this diagnosis is intelligent guess-work.
The remainder of the problem statements are listed in an order the nurse judges to be correct. In this situation the nurse has listed the infection as second in urgency. It is, (based upon the CBC) an acute infection and Mrs. R needs to have her antibiotics started ASAP.
The third problem statement is listed as impaired nutrition. Physiologically a more urgent need than "Safety", but it is obviously a chronic problem. It did not develop within the last few days.
The fourth problem is impaired safety related to Mrs. R's depressed sensorium. If this is "metabolic" in origin, it will clear as the other needs (fluid, infection control and nutrition) are resolved. The nurse does not know what Mrs.R's best baseline mentation is and clearly indicates that some parts of this diagnosis is intelligent guess-work.
Goal Statements: The simplest goal statements are those that (reverse) mirror the assessments. If part of the assessment leading to a problem statement is fever, then obviously, if planned actions are effective, the fever should resolve. This is clearly seen in the goal statements for problems. Because the nurse does not know what Mrs. R's baseline mentation is, it is more difficult to write a goal statement for the last problem. Nevertheless, all the goal statements are patient oriented, in a time context, and quantifiable or binary.
Nursing Actions: The nursing actions for problem 1 are both collaborative and independent. The most definitive way to hydrate a lethargic patient is to do it IV. So the physican's order for IV fluids is listed first. The nurse also anticipated being able to hydrate the patient by mouth. (See evaluation/reformulation below.) The patient's mouth and mucous membranes were in very bad shape due to dehydration and neglect when the patient arrived. The nurse puts a priority on getting these tissues clean and keeping them that way. The remaining nursing actions for this problem are aimed at monitoring both intake and output. However, since an indwelling catheter would expose Mrs. R. to infection (and a hospital acquired one at that...) the measurements of output can only be semiquantifiable. Similarly for problem 2, the actions are both collaborative and independent. The patient needs to have antibiotics to treat her infection and that is shown here. Other related nursing actions are related to monitoring. Nursing actions for problem 3 recognize that Mrs. R. is at risk of refeeding syndrome if she is nourished to well too quickly. (See below)
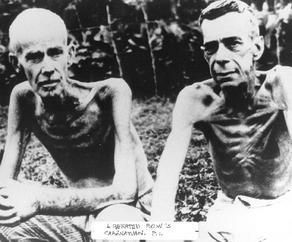
Refeeding Syndrome: There is a condition called “refeeding syndrome” and we learned about it in a very unfortunate way. GI’s who were imprisoned by the Japanese were severely malnourished. Once released, the former POW’s were given food with the best of intensions, but it killed them instead of helping them.
Refeeding syndrome occurs because mitochondria have (in starvation) run perilously low on phosphate supplies trying to generate ATP without adequate glucose. Once glucose is rushed back into the body, the mitochondria begin generating ATP at a rapid pace, quickly running out of phosphate. This causes catastrophic collapse of metabolic substrate, and massive cellular death. We know D.K. is at risk of re-feeding syndrome because her serum Mg2+ and PO4- are low.
Refeeding syndrome occurs because mitochondria have (in starvation) run perilously low on phosphate supplies trying to generate ATP without adequate glucose. Once glucose is rushed back into the body, the mitochondria begin generating ATP at a rapid pace, quickly running out of phosphate. This causes catastrophic collapse of metabolic substrate, and massive cellular death. We know D.K. is at risk of re-feeding syndrome because her serum Mg2+ and PO4- are low.
